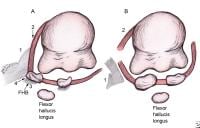
In the 19th century, the prevalent understanding of the bunion—hallux valgus—was that it was purely an enlargement of the soft tissue, first metatarsal head, or both, most commonly caused by ill-fitting footwear. Thus, treatment had varying results, with controversy over whether to remove the overlying bursa alone or in combination with an exostectomy of the medial head. These surgeries were considered to be beneath many surgeons, so the understanding of the pathology of hallux valgus was gradual in its development. Surgeons slowly began to recognize that bunions could develop as a result of numerous different factors, that they tended to be familial, and that they often were associated with other foot deformities.
 As the school of thought began to shift, the first surgical treatment to address deforming pathology was developed and presented on May 4, 1881, when J. L. Reverdin gave a report on hallux abductovalgus to the Medical Society of Genfer. He described a procedure in which a curved incision medial to the extensor hallucis longus was followed by incision of the periosteum, chiseling off of the exostosis, removal of a wedge of bone from behind the capitulum of the metatarsus, and suturing of the bone with catgut. This operation is considered to be the forerunner of all operations that aim to correct hallux valgus via osteotomy.
As the school of thought began to shift, the first surgical treatment to address deforming pathology was developed and presented on May 4, 1881, when J. L. Reverdin gave a report on hallux abductovalgus to the Medical Society of Genfer. He described a procedure in which a curved incision medial to the extensor hallucis longus was followed by incision of the periosteum, chiseling off of the exostosis, removal of a wedge of bone from behind the capitulum of the metatarsus, and suturing of the bone with catgut. This operation is considered to be the forerunner of all operations that aim to correct hallux valgus via osteotomy. Preoperative radiograph.
Preoperative radiograph. Postoperative radiograph shows Keller, or resectional, arthroplasty.
Postoperative radiograph shows Keller, or resectional, arthroplasty. Preoperative radiograph shows degenerative joint disease.
Preoperative radiograph shows degenerative joint disease. Postoperative radiograph obtained after resectional arthroplasty and total joint implant placement.
Postoperative radiograph obtained after resectional arthroplasty and total joint implant placement. Preoperative template for implant placement.
Preoperative template for implant placement.Since its inception, the Reverdin procedure has undergone many variations and modifications, including the addition of lateral releases and proximal osteotomies, in an effort to address deformity. Indeed, more than 100 procedures have been attempted and developed for the correction of hallux valgus. However, many of these variations have been developed out of ignorance; some are even repetitions of previous procedures, both failed and successful. Surgeons have continued to reevaluate the osteotomy in search of the most stable procedure with the fewest complications.
Recent studies
Shima et al investigated the intraobserver and interobserver reliability of different radiographic methods used to measure the hallux valgus and intermetatarsal angles and to determine the most reliable method for making those measurements before and after a proximal crescentic osteotomy of the first metatarsal. The method that yielded the highest intraobserver and interobserver correlation coefficients for the preoperative hallux valgus and intermetatarsal angles and the postoperative hallux valgus angle was that in which a line connected the centers of the first metatarsal head and the proximal articular surface of the first metatarsal to define the longitudinal axis of the first metatarsal. The authors therefore recommended that this method be used for evaluating radiographs before and after a proximal crescentic osteotomy for the treatment of hallux valgus.[1]
Schuh et al studied the changes of plantar pressure distribution during the stance phase of gait in patients who underwent hallux valgus surgery followed by a multimodal rehabilitation program. The study included 30 patients who underwent Austin and scarf osteotomy for correction of mild to moderate hallux valgus deformity and began a rehabilitation program 4 weeks postoperatively (once per week for 4-6 wk). Plantar pressure analysis was performed preoperatively and at 4 weeks, 8 weeks, and 6 months postoperatively. Range of motion of the first metatarsophalangeal joint was also measured.[2]
The results of the Schuh study included an increased mean American Orthopaedic Foot and Ankle Society (AOFAS) score rom 60.7 points preoperatively to 94.5 points 6 months after surgery, and the first metatarsophalangeal joint range of motion increased at 6 months, with a significant increase in isolated dorsiflexion. In the first metatarsal head region, maximum force increased from 117.8 N to 126.4 N, and the force-time integral increased from 37.9 N.s to 55.6 N.s. In the great toe region, maximum force increased from 66.1 N to 87.2 N, and the force-time integral increased from 18.7 N.s to 24.2 N.s
0 komentar:
Post a Comment